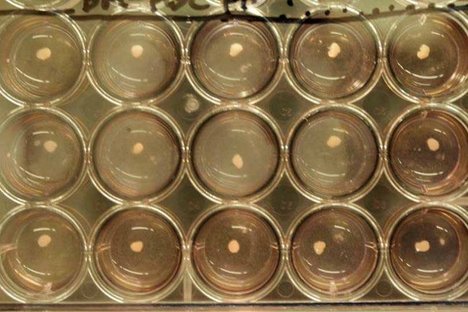
 “Researchers from Japan used human stem cells to create “liver buds,” rudimentary livers that, when transplanted into mice, grew and functioned.” Source of caption and photo: online version of the NYT article quoted and cited below.
“Researchers from Japan used human stem cells to create “liver buds,” rudimentary livers that, when transplanted into mice, grew and functioned.” Source of caption and photo: online version of the NYT article quoted and cited below.
(p. A3) Researchers in Japan have used human stem cells to create tiny human livers like those that arise early in fetal life. When the scientists transplanted the rudimentary livers into mice, the little organs grew, made human liver proteins, and metabolized drugs as human livers do.
They and others caution that these are early days and this is still very much basic research. The liver buds, as they are called, did not turn into complete livers, and the method would have to be scaled up enormously to make enough replacement liver buds to treat a patient. Even then, the investigators say, they expect to replace only 30 percent of a patient’s liver. What they are making is more like a patch than a full liver.
But the promise, in a field that has seen a great deal of dashed hopes, is immense, medical experts said.
“This is a major breakthrough of monumental significance,” said Dr. Hillel Tobias, director of transplantation at the New York University School of Medicine. Dr. Tobias is chairman of the American Liver Foundation’s national medical advisory committee.
For the full story, see:
GINA KOLATA. “Scientists Fabricate Rudimentary Human Livers.” The New York Times (Thurs., July 4, 2013): A3.
(Note: the online version of the story has the date July 3, 2013.)