Source of graphic: online version of the NYT article quoted and cited below.
Source of graphic: online version of the NYT article quoted and cited below.
Why are so many lumbar fusions done, in spite of the absence of evidence for their efficacy? Well, doctors find the procedure lucrative. Patients do not pay for it themselves, so they have little incentive to look hard at the effectiveness. And health care providers, through licensing and government regulations, have largely insulated themselves from competition from low cost providers.
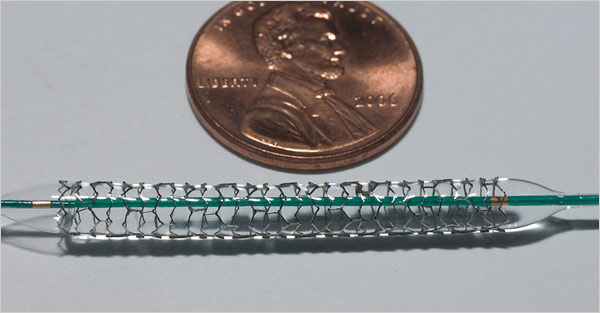
(p. C1) In Idaho Falls, Idaho, anyone suffering from the sort of lower back pain that may conceivably be helped by the fusing of two vertebrae is quite likely to have the surgery. It’s known as lumbar fusion, and the rate at which it is performed in Idaho Falls is almost five times the national average. The rate in Idaho Falls is 20 times that in Bangor, Me., where lumbar fusion is less common than anywhere else.
These numbers come from the wonderful Dartmouth Atlas of Health Care. The Dartmouth researchers adjust the numbers to take into account age, race and sex, which is another way of saying that there is no good explanation for the huge variations they find. Doctors in the Idaho Falls area are probably just being more aggressive than doctors elsewhere.
But it’s not clear that their patients are any better off. The evidence for lumbar fusion is incredibly mixed. It seems to help people with certain kinds of pain, but many others recover just as well without the surgery. Of course, doctors are almost always better off if the surgery is done: The typical hospital bill for lumbar fusion is roughly $50,000.
This is about as good an example as you can find of the health care mess. The number of lumbar fusions performed in this country has more than tripled since the early 1990s, and Medicare now spends more than $600 million a year on the procedure. It’s one reason your health insurance bill has gone up.
For the full commentary, see:



 A CVS pharmacy MinuteClinic. Source of photo: online version of the WSJ article cited below.
A CVS pharmacy MinuteClinic. Source of photo: online version of the WSJ article cited below.  Source of graphic: online version of the NYT article quoted and cited below.
Source of graphic: online version of the NYT article quoted and cited below.